
Lianne – Cancer Today Magazine
This article was originally published on cancertodaymag.org on December 11, 2025 and was written by Kendall K. Morgan.
Rethinking Brain Metastases
With the option for targeted treatment and radiation, more people with stage IV cancer are being spared from whole-brain radiation.
WHEN 37-YEAR-OLD SPEECH language pathologist Lianne Kraemer of Chicago was diagnosed with stage II hormone receptor-positive breast cancer in January 2014, she had a double mastectomy followed by chemotherapy and radiation. She was preparing to take hormone therapy to lower her estrogen levels and reduce her risk of recurrence when, in June 2016, she felt a strange sensation on the right side of her face.
“It was like a light switch,” she says. “I was standing in front of the dryer, and it was like someone flipped a switch and my face became tingly.”
Within 24 hours, the tip of her right index finger started tingling too. She received an MRI scan, which revealed 12 spots in her brain. Subsequent bone and CT scans offered some good news: She had no signs of cancer anywhere else in her body.
“It was a very strange thing to be saying, ‘Well, thank God it’s only in my brain,’” Kraemer says.
Targeting the Brain
Hormone receptor-positive breast cancer typically spreads to other areas, such as the bones, before spreading to the brain. “In the early-stage breast cancer setting, having a central nervous system-only recurrence is not super common, but once people have metastatic disease, if you follow them over time, it does become quite common,” says Nancy Lin, a breast oncologist at Dana-Farber Cancer Institute in Boston.
Brain metastases are more common in HER2-positive or triple-negative breast cancers. As many as half of those with advanced HER2-positive breast cancer will have brain metastases, Lin says. At least 1 in 4 people with advanced triple-negative breast cancer will have brain metastases. For those with metastatic hormone receptor-positive breast cancer, the chance of cancer spreading to the brain is closer to 1 in 10. Even so, 80% of breast cancer diagnoses are categorized as hormone receptor-positive, which makes brain metastases in this subtype relatively common.
Each year, approximately 200,000 people will be diagnosed with cancer that has metastasized to the brain. Brain metastases are more common in some cancer types, such as lung cancer and melanoma. Just a few decades ago, people with brain metastases generally weren’t expected to live more than six months, and brain metastases were long treated as a medical emergency using a one-size-fits-all approach, according to Christopher Anker, a radiation oncologist at the University of Vermont Cancer Center in Burlington.
Twenty years ago, radiation oncologists could receive calls in the middle of the night or on weekends about patients with newly diagnosed brain metastases, asking them to come see the patient immediately, then start radiation therapy within 24 hours—often to the whole brain, Anker says. “The dogma was that chemo doesn’t work in the brain, so radiation therapy was essential.”
Dramatic Changes
Now, targeted approaches have provided additional options that can reduce the risk of cognitive problems that can come with whole-brain radiation, says Priscilla Brastianos, a neuro-oncologist at Mass General Brigham Cancer Institute in Boston. While there’s still a need for more approaches to prevent and treat brain metastases, Brastianos says, “over the past decade, things have changed dramatically.”
Given the number of new treatments, the American Society for Radiation Oncology provided guidance in 2022 to break down approaches and evidence for managing brain metastases. In that review, experts noted that stereotactic radiosurgery, which delivers narrow high-dose beams of radiation straight to the tumors, can provide tumor control when brain metastases are limited and even in some patients who have five to 10 small growths.
Systemic treatments have also provided more options for patients. For example, some targeted therapies, such as EGFR inhibitors for non-small cell lung cancer (NSCLC), appear to penetrate the protective shield around the brain called the blood-brain barrier. Immune checkpoint inhibitors, which can help activate a person’s T cells to fight cancer, also have been shown to control metastatic growths in the brain. More recently, an antibody-drug conjugate (ADC) called Enhertu (trastuzumab deruxtecan), which uses an antibody that binds to proteins on the cancer cell and delivers chemotherapy straight to tumors, has also curbed cancer growth in the brain for people with HER2-positive breast cancer.
“We have three types of treatments for brain metastases: surgery, radiation and some sort of systemic therapy,” Lin says. “Which is chosen, and in which order, really depends a lot on individualizing things for the patients.”
Thus, a person with stable metastatic breast cancer could receive stereotactic radiosurgery to treat two small growths in the brain, Lin says, while others who have cancer with certain molecular markers may find that targeted therapies can control brain metastases. “In that situation, we might ordinarily be thinking about whole-brain radiation treatment, but let’s suppose [their cancer is] HER2-positive and they’ve never had Enhertu before. That’s a patient where the response rate to the systemic treatment is very high—over 80%—and the upside is to spare people the need for whole-brain radiation therapy,” says Lin.
A Systemic Approach
The Food and Drug Administration first approved Enhertu in 2019 for unresectable or metastatic breast cancer that expresses HER2. As research evolves on this treatment, the DESTINY-Breast12 clinical trial, published Sept. 13, 2024, in Nature Medicine, assessed the use of Enhertu in 263 people with HER2-positive breast cancer and brain metastases. In the study, 61.6% of patients with brain metastases had no disease growth at one year. The findings showed that Enhertu works to control cancer not only in the body but also in the brain, says Lin.
The study wasn’t the first to show systemic treatments could control brain metastases in HER2-positive breast cancer, Lin says. A 2020 trial, dubbed HER2CLIMB, found adding Tukysa (tucatinib) to Herceptin (trastuzumab) and the oral chemotherapy Xeloda (capecitabine) could increase survival and time to progression in people with brain metastases. After two and a half years, people taking Tukysa, Xeloda and Herceptin lived a median of 9.1 months longer than those taking a placebo, Xeloda and Herceptin. The trial also found that people taking Tukysa, which is a small-molecule tyrosine kinase inhibitor that blocks part of the HER2 receptor, were less likely to develop new lesions in the brain.
Immunotherapy has also shown promise in controlling brain metastases. For instance, one 2021 research analysis that included 171 people with NSCLC and brain metastases found a median overall survival of 18.8 months in those who received Keytruda (pembrolizumab) plus chemotherapy, compared with 7.6 months for those who took chemotherapy alone. The median progression-free survival with and without immunotherapy was 6.9 months and 4.1 months, respectively.
It remains important to gather evidence to improve treatments for people with other brain metastases “outside the big areas of lung cancer, melanoma and breast cancer,” Lin says.
To build on progress, clinical trials should continue to include people with brain metastases, Brastianos says. But an important shift in mindset has already taken place. “We no longer assume that everything must be managed with radiation alone,” she says. “Instead, we are combining systemic therapies with local treatments, including surgery and radiation, in ways that are thoughtful and evidence based.”
Continued Progress
As a researcher, Brastianos spends much of her time exploring how and why cancers spread to the brain in the first place. She is studying how acquired genetic changes in the primary cancer allow them to infiltrate and take up residence in the brain. She is leading a phase II clinical trial exploring how genetic changes in metastatic brain tumor samples from people with lung, breast and other cancers could be used to determine effective systemic therapies.
Anker is leading a small trial at the University of Vermont Cancer Center to determine whether people with brain metastases that respond to systemic therapies, including immunotherapy and targeted therapy, can safely avoid radiosurgery. The trial will enroll 45 people with brain metastases—30 with NSCLC and 15 with other primary cancers—whose treatment plan includes targeted therapy, immunotherapy or a combination of both. Anker designed the trial after he observed many patients taking systemic therapy that controlled their brain metastases who were planning to receive radiosurgery.
“It became exciting to say, ‘You don’t necessarily need to treat this with radiation; it’s already responding. What do you think about watching these instead?’” Anker says.
Advertisement
While radiation was once an automatic treatment for people with brain metastases, radiologists and oncologists now consider each case individually, he says. Sixty-year-old Mike Rock, who was diagnosed with stage IV NSCLC in April 2025, was the first person to enroll in Anker’s trial. By the time he received his diagnosis, his cancer had already spread to his bones and liver. An MRI also revealed one spot on his brain. Anker told Rock he had a choice to make. They could treat the tumor in his brain with radiation right away, or he could consider the clinical trial to see if systemic therapy might work on its own. Rock says he thought the trial was a “good bet” and enrolled.
While waiting to receive results from tumor testing, Rock started chemotherapy treatment. When his tumor didn’t test positive for any mutations that could qualify him for targeted therapy, Rock started taking the immunotherapy drug Keytruda in April 2025 along with the chemotherapy treatment—a combination that led to “truly dramatic” scans with Rock’s brain tumor disappearing, Anker says. Rock is excited to be a part of research that could help other patients avoid unnecessary radiosurgery treatments and complications, such as necrosis, which occurs when normal brain tissue surrounding the tumor dies. His systemic treatment with immunotherapy and chemotherapy could also be controlling brain metastases that are still too small to show up on scans, Anker says.
For Kraemer, who had numerous brain metastases in 2016, the obvious treatment regimen was whole-brain radiation. However, her medical oncologist suggested that she enroll in a clinical trial that was testing an experimental drug called abemaciclib in people with brain metastases, including those with breast cancer. The drug blocked the activity of two proteins, CDK4 and CDK6, that can lead to uncontrolled cancer growth.
Kraemer was worried about the effects of whole-brain radiation and opted for the trial. (Later, seeking a second opinion, she found Lin, who was enrolling patients in that same trial.)
An MRI at six weeks showed her brain tumors were stable. She had side effects, including chronic diarrhea, which led her to take a lower dose of the medication. When her cancer started to progress in early 2017, she was no longer eligible to participate in the clinical trial, but she was able to arrange to receive abemaciclib from the drug company. Her doctor also added hormone therapy to the regimen. (The Food and Drug Administration would go on to approve abemaciclib under the brand name Verzenio in 2017 for people with advanced or metastatic hormone receptor-positive, HER2-negative breast cancer.)
The abemaciclib and hormone therapy kept her brain metastases in check for a year until June 2018. In the years since, she has followed a combined approach to treatment, taking hormone therapy along with a long series of intravenous chemo and other oral chemotherapy drugs, including Xeloda. She has also received radiosurgery for tumors in sensitive areas of her brain, such as one that appeared near her optic nerve. “What I have is not a chronic disease, but we treat it as if it were,” Kraemer says.
Now almost a decade since Kraemer was diagnosed with advanced breast cancer, her experience challenges assumptions about what it means to live with brain metastases. While she can no longer work as a speech language pathologist, she uses her experience to offer guidance to others living with incurable cancer. She has teamed up with patient advocacy organizations, such as the Metastatic Breast Cancer Alliance, to push for increased funding for metastatic breast cancer research, as well as changes to how doctors screen for brain metastases. She also worked alongside researchers to help shape the 2022 American Society for Radiation Oncology guidelines on radiation therapy for brain metastases. Lin sees Kraemer’s example and the evolving story in metastatic breast cancer as a hopeful example for what’s possible in other solid cancers.
“What the story in metastatic breast cancer tells us is that, if we actually make an effort and try to develop drugs for patients who have brain metastases, it really makes a big difference,” Lin says. “There has been such a nihilism about brain metastases, and it becomes this sort of self-fulfilling prophecy. But the minute you actually try to put in resources and you try new treatments, some things work, and they can really make a tremendous difference in the lives of patients.”













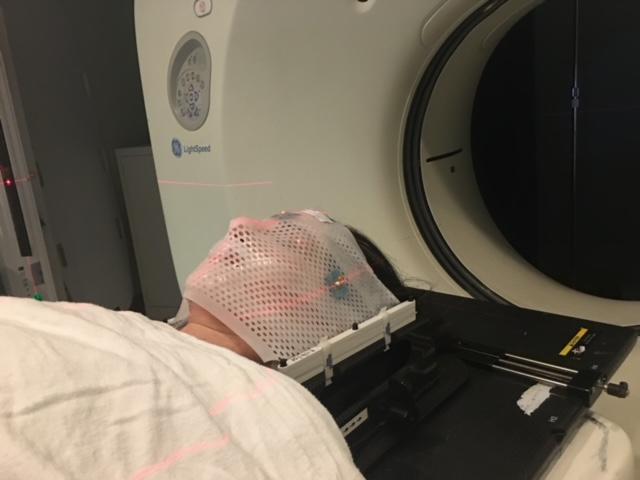 Getting the mask made was no picnic. I felt it hard to breathe and swallow and couldn’t wait to get it off.I got used to it pretty fast, which is lucky for me since I’ve used it multiple times since that first time. This is a picture of me right before my first SRS radiation. I was nervous about the side effects, but otherwise, I was comfortable and okay with the mask. I can imagine that claustrophobic people may have a hard time getting used to this.
Getting the mask made was no picnic. I felt it hard to breathe and swallow and couldn’t wait to get it off.I got used to it pretty fast, which is lucky for me since I’ve used it multiple times since that first time. This is a picture of me right before my first SRS radiation. I was nervous about the side effects, but otherwise, I was comfortable and okay with the mask. I can imagine that claustrophobic people may have a hard time getting used to this.
